Parasitology

Parasitology
More Posts from T-b-a-blr-blog and Others
Hi optom! I'm very new to the studyblr community and it's my first term of university. I was a straight A student in high school and i am not performing well in my classes. In fact... I'm doing terribly. About a B to B- average. I know I'm probably not the first to go through so I've been trying to find posts that help students cope with this. Resources. Helpful tips. Is there a tag you can recommend? Any posts that you've encountered/wrote that I could peruse? Thank you very much for any help!
Hey there, thanks for asking. This is actually a very common problem experienced by people as they progress from high school to university.
The problem is that mediocre study techniques and a combination of natural ability may have gotten you straight As whilst in high school, but it’s just not going to cut it in university. Cracking down on yourself and sitting down for more hours isn’t going to make your grades much better; it’s just doing more of the same mediocre studying.
So you basically need to read up on good studying techniques and actually apply them to your studies.
Everything You Need to Cover To Succeed As A Student
I actually have a web directory of all my study tips which already lists all these links.
So because the problem you have at its base is most likely that you’re using high school level techniques to tackle university-level problems, you’ll need to find resources on all areas related to good studying. For some of these areas, I have a related post, but for the more generalised topics like procrastination, I haven’t yet put one out because if I do, I want to be certain that the post will be unique, useful and practical.
Without further ado, here’s a list of all the tags/areas you should work through and evaluate whether you need to change your current study habits if you want to be a 4.0/HD student at university.
Firstly, have a read of my recent answer about 20 Things You Can Do To Prepare for University, and click through to any of the parts of my 15-Part University 101 Series.
Time management
Organisation (see Part 3 Studying and Part 8 Four Secrets from University and Part 11 Adapting to Uni Studying which covers how you can manage university workloads on the whole and specific changes to your studies you should make)
Motivation
Discipline / Staying Focused
Procrastination (see post by @samsstudygram)
Study Methods (I’ve got one on the Blank Paper Method and the Cornell Method)
Exams (I’ve got a multi-part series in the works)
Study Materials (see Part 2 of my University Series for some tips)
Studying from Textbooks (see Part 12 How To Study From Textbooks in Uni which deals with this specifically)
Self Care (you can see my tag here of my own + useful curated posts)
Spaced Repetition (use Anki!)
Study Space (I have a masterpost with tips here)
Hope that helps! If you have a specific question about any areas then let me know!

Me durning finals.
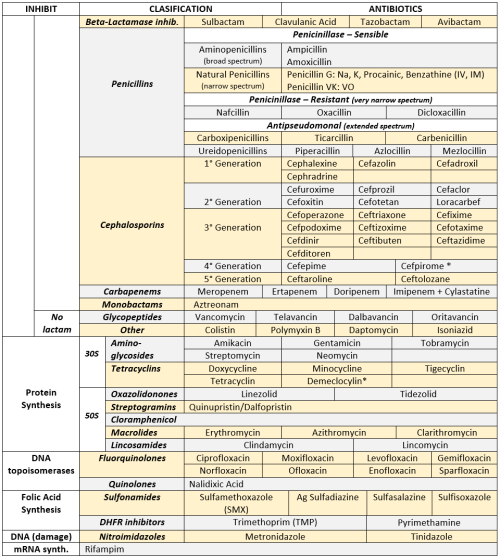
ANTIBIOTICS CHEAT SHEET :)
Also, REMEMBER!!!!
* Sulfonamides compete for albumin with:
Bilirrubin: given in 2°,3°T, high risk or indirect hyperBb and kernicterus in premies
Warfarin: increases toxicity: bleeding
* Beta-lactamase (penicinillase) Suceptible:
Natural Penicillins (G, V, F, K)
Aminopenicillins (Amoxicillin, Ampicillin)
Antipseudomonal Penicillins (Ticarcillin, Piperacillin)
* Beta-lactamase (penicinillase) Resistant:
Oxacillin, Nafcillin, Dicloxacillin
3°G, 4°G Cephalosporins
Carbapenems
Monobactams
Beta-lactamase inhibitors
* Penicillins enhanced with:
Clavulanic acid & Sulbactam (both are suicide inhibitors, they inhibit beta-lactamase)
Aminoglycosides (against enterococcus and psedomonas)
* Aminoglycosides enhanced with Aztreonam
* Penicillins: renal clearance EXCEPT Oxacillin & Nafcillin (bile)
* Cephalosporines: renal clearance EXCEPT Cefoperazone & Cefrtriaxone (bile)
* Both inhibited by Probenecid during tubular secretion.
* 2°G Cephalosporines: none cross BBB except Cefuroxime
* 3°G Cephalosporines: all cross BBB except Cefoperazone bc is highly highly lipid soluble, so is protein bound in plasma, therefore it doesn’t cross BBB.
* Cephalosporines are "LAME“ bc they do not cover this organisms
L isteria monocytogenes
A typicals (Mycoplasma, Chlamydia)
M RSA (except Ceftaroline, 5°G)
E nterococci

* Disulfiram-like effect: Cefotetan & Cefoperazone (mnemonic)
* Cefoperanzone: all the exceptions!!!
All 3°G cephalosporins cross the BBB except Cefoperazone.
All cephalosporins are renal cleared, except Cefoperazone.
Disulfiram-like effect
* Against Pseudomonas:
3°G Cef taz idime (taz taz taz taz)
4°G Cefepime, Cefpirome (not available in the USA)
Antipseudomonal penicillins
Aminoglycosides (synergy with beta-lactams)
Aztreonam (pseudomonal sepsis)
* Covers MRSA: Ceftaroline (rhymes w/ Caroline, Caroline the 5°G Ceph), Vancomycin, Daptomycin, Linezolid, Tigecycline.
* Covers VRSA: Linezolid, Dalfopristin/Quinupristin
* Aminoglycosides: decrease release of ACh in synapse and act as a Neuromuscular blocker, this is why it enhances effects of muscle relaxants.
* DEMECLOCYCLINE: tetracycline that’s not used as an AB, it is used as tx of SIADH to cause Nephrogenic Diabetes Insipidus (inhibits the V2 receptor in collecting ducts)
* Phototoxicity: Q ue S T ion?
Q uinolones
Sulfonamides
T etracyclines

* p450 inhibitors: Cloramphenicol, Macrolides (except Azithromycin), Sulfonamides
* Macrolides SE: Motilin stimulation, QT prolongation, reversible deafness, eosinophilia, cholestatic hepatitis
* Bactericidal: beta-lactams (penicillins, cephalosporins, monobactams, carbapenems), aminoglycosides, fluorquinolones, metronidazole.
* Baceriostatic: tetracyclins, streptogramins, chloramphenicol, lincosamides, oxazolidonones, macrolides, sulfonamides, DHFR inhibitors.
* Pseudomembranous colitis: Ampicillin, Amoxicillin, Clindamycin, Lincomycin.
* QT prolongation: macrolides, sometimes fluoroquinolones

Ketone bodies are produced in the liver and can be used as an energy source in the mitochondrial of peripheral tissues. Important fact: RBCs can not use ketones because they lack mitochondria.
The liver is unable to peform Ketolysis because it lacks Thiophorase (Succinyl-CoA Acetoacetate Transferase), and is hence unable to activate its own ketones.

New background! Download higher quality photo here!
https://drive.google.com/file/d/1F5SlJmB8YiNNtGuKrc-QtMnrrjZ1tOHL/view?usp=sharing
Live, attenuated Vaccines Available in the US
Live vaccines induce HUMORAL & CELL-MEDIATED immunity
MRS. V.Z. FYI MAP

M umps / M easles
R ubella
S mallpox
.
V aricella Z oster
.
F rancisella tularensis
Y ellow Fever
In fluenza (intranasal)
.
M icobaterium bovis (BCG)
A denovirus
P olio (sabin)

One possible cover design for The Book
Coming soon.
What is Acute or Subacute Bacterial Endocarditis?
Acute or Subacute Bacterial Endocarditis is an infection of the heart’s endocardium. The endocardium is the inner lining of the heart muscle, which also covers the heart valves. Bacterial Endocarditis can damage or even destroy your heart valves. The difference between acute and subacute bacterial endocarditis is acute bacterial endocarditis is a sudden onset, whereas subacute bacterial endocarditis is a gradual onset.
Acute endocarditis most often occurs when an aggressive species of skin bacteria, especially a staphylococcus (staph), enters the bloodstream and attacks a normal, undamaged heart valve. Once staph bacteria begin to multiply inside the heart, they may send small clumps of bacteria called septic emboli into the bloodstream to spread the infection to other organs, especially to the kidneys, lungs and brain. Intravenous (IV) drug users are at very high risk of acute endocarditis, because numerous needle punctures give aggressive staph bacteria many opportunities to enter the blood.If untreated, this form of endocarditis can be fatal in less than six weeks.
Subacute endocarditis is caused by one of the viridans group of streptococci (Streptococcus sanguis, mutans, mitis or milleri) that normally live in the mouth and throat. Streptococcus bovis or Streptococcus equinus also can cause subacute endocarditis, typically in patients who have some form of gastrointestinal cancer, usually colon cancer. Subacute endocarditis tends to involve heart valves that already are damaged in some way, and it usually is less likely to cause septic emboli than acute endocarditis. If untreated, subacute bacterial endocarditis can worsen for as long as one year before it is fatal.
![[x]](https://64.media.tumblr.com/955b3402836e292187e6435c26797c9d/tumblr_ohsjpvHnW61qiz5q7o1_500.jpg)
[x]
If you cannot grasp what I have just explained, you should just leave and study economics!
Microbiology professor, first lecture (via scienceprofessorquotes)
-
 paureus reblogged this · 5 years ago
paureus reblogged this · 5 years ago -
 doctornimsblog liked this · 6 years ago
doctornimsblog liked this · 6 years ago -
 t-b-a-blr-blog reblogged this · 6 years ago
t-b-a-blr-blog reblogged this · 6 years ago -
t-b-a-blr-blog liked this · 6 years ago
-
 vachonski-blog liked this · 7 years ago
vachonski-blog liked this · 7 years ago -
 adilamkarol liked this · 7 years ago
adilamkarol liked this · 7 years ago -
 raons liked this · 7 years ago
raons liked this · 7 years ago -
 zhuykay-blog reblogged this · 8 years ago
zhuykay-blog reblogged this · 8 years ago -
zhuykay-blog reblogged this · 8 years ago
-
 whitewingfeathers reblogged this · 8 years ago
whitewingfeathers reblogged this · 8 years ago -
whitewingfeathers liked this · 8 years ago
-
 befitbeautifulandhappy liked this · 8 years ago
befitbeautifulandhappy liked this · 8 years ago -
miscmona-blog reblogged this · 9 years ago
-
miscmona-blog liked this · 9 years ago
-
mymltnotes liked this · 11 years ago
-
 schwann86-blog reblogged this · 11 years ago
schwann86-blog reblogged this · 11 years ago -
 nadhk reblogged this · 12 years ago
nadhk reblogged this · 12 years ago -
 bucketbaby liked this · 12 years ago
bucketbaby liked this · 12 years ago -
 misbehavingmyself liked this · 12 years ago
misbehavingmyself liked this · 12 years ago -
 about-hortense liked this · 12 years ago
about-hortense liked this · 12 years ago -
 cherrierenee liked this · 12 years ago
cherrierenee liked this · 12 years ago -
 mynotes4usmle reblogged this · 12 years ago
mynotes4usmle reblogged this · 12 years ago
